
The Unified
Model of OCD draws on clinical and academic research conducted over the last 75
years to present an integrated understanding of the different cognitive and
behavioural factors that maintain Obsessive Compulsive Disorder.
This
includes psychological concepts from the original OCD Phobic Model, Exposure
and Response Prevention (ERP), Inhibitory Learning, the Cognitive Appraisal
Model, Metacognitive Therapy, Acceptance and Commitment Therapy and more recently, Inference Based Therapy.
Whilst the
concepts covered in these different approaches are numerous and complex, the
Unified Model integrates these distinct contributions into a simple four-part model. This provides a coherent basis for integrating the latest research into
Obsessive Compulsive Disorder, whilst providing flexible access to the best
treatment options from these different models.
Note: The following information provides a
detailed understanding of the psychological processes behind the OCD
cycle. It should however be noted that clients would not normally be expected
to read and immediately understand these processes without the support and
assistance of a properly qualified professional.
Our specialist OCD treatments are led and supervised by William Phillips, our Principal Psychotherapist. In addition to his work at GoodCBT.com, William consults with a number of other private clinics and provides clinical supervision to other Psychologists and Cognitive Behavioural Psychotherapists. You can learn more about William here.
Whilst a
number of different OCD presentations and subtypes have been identified over
the years, all forms of OCD follow the same basic psychological pattern. This
is presented as a four-part process involving relevant background factors, triggers / intrusions, obsessional doubts and compulsive / avoidance behaviours:
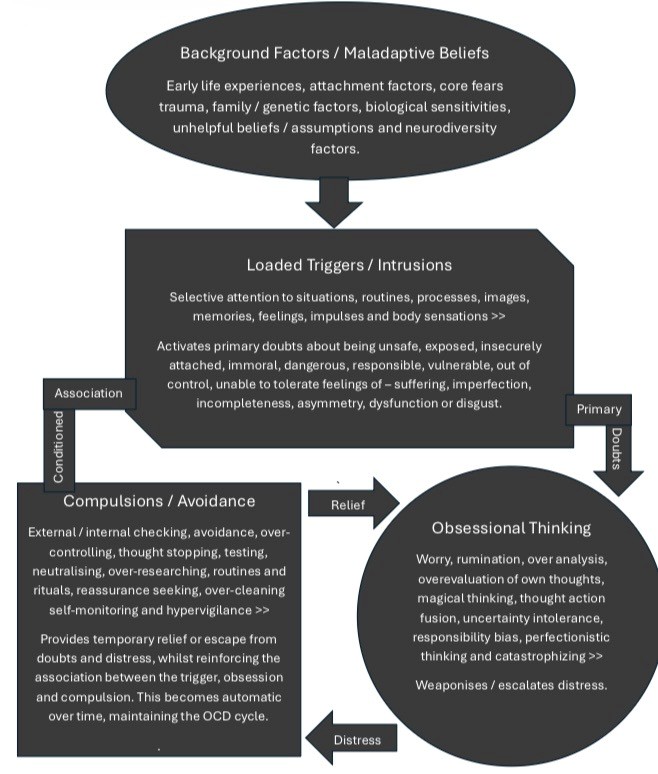
Whilst Obsessive Compulsive Disorder is maintained by a number of faulty thinking patterns and compulsive behaviours, research indicates that early life experiences, family, genetic, trauma-related, cognitive and behavioural factors can act as predisposing factors in the development of OCD. Identifying and where appropriate, addressing some of these background factors may support effective treatment. This is particularly relevant where early formed maladaptive beliefs, irrational assumptions and unresolved traumatic experiences continue to maintain the individual's vulnerability to OCD doubts.
This
initial phase is represented in the folded edge “Rectangle” shape at the top of
the OCD model.
In this
phase, hypervigilant scanning and selective attention to internal or external
cues, cause normal doubts or hypothetical possibilities to be automatically
interpreted as potential threats or dangers.
Triggers or
OCD cues can include situations, events, images, memories, feelings and body
sensations.
Over time
and through the processes of operant learning, classical conditioning and
inferential confusion, these normal triggers become synonymous with a “Primary
Doubt”. E.g. leaving the house and being responsible for a break-in or house
fire. Touching a door handle and being contaminated by germs or chemicals.
Noticing an attractive person and doubting one’s own sexual preferences. Seeing
a child and fearing perverse or shameful intentions.
The problem
is, that the primary doubt becomes tacit and automatic, passing from the
trigger stage into the obsessional doubting stage, where it is supercharged and
weaponized to such an extent that it leads to intolerable levels of distress.
Whilst the
psychological processes of operant and conditioned learning have long been
acknowledged as behavioural factors in the development of OCD, research into a
special form of cognitive therapy known as Inference Based Therapy (IBT), has
also identified problems with the psychological processes of internal doubting,
as a significant aspect in the maintenance of OCD. This process of “Inferential
Confusion” which is relatively new in the field of OCD treatment, deserves it’s
own brief footnote:
In addition
to the behavioural affects of operant learning and classical conditioning,
(covered in the second and third phases of our cycle ), the “Primary Doubt” is established and
strengthened through a psychological process known as “Inferential Confusion”.
This is an
automatic cognitive process taking place
at the initial phase of the cycle. It involves an abandonment of the evidence
and an over investment in remote or imagined possibilities at the cost of the
individual’s own common sense.
To
understand how this works, we need to draw the distinction between external
rational doubts and internal irrational doubts.
External rational
doubts are normal uncertainties based on balanced and observable data. So for
example we might pause to consider our forgotten umbrella when dashing for a
late meeting and noticing dark clouds in the sky. Do we go back for the
umbrella which may cause further delays, or do we take the chance of turning up
to our meeting wet through and soggy?
When we
make healthy judgements or gambles about normal external and observable
uncertainties, we refer to this as rational doubt.
On the flip
side, irrational doubts involve automatically abandoning the evidence and
established common sense in support of internally imagined possibilities.
Drawing on
the clouds and umbrella metaphor, not only do we over estimate the chances of
getting wet when the forecast is clear and dry, we might “magically” and
tacitly associate the absence of our umbrella with the increased likelihood of
rain.
In our OCD
model, the “Primary Doubt” is always an irrational, internally synthesized doubt synonymous with a normal or ordinary
trigger.
The problem
is that this process becomes automatic and pervasive over time. It passes
unnoticed or unchallenged from the first trigger phase into the second
obsessional phase. It slips under the radar of conscious awareness into the
obsessional phase of the OCD cycle, where it is inadvertently validated and
reinforced through obsessional thinking and compulsive behaviour.
Once the
“Primary Doubt” passes into the obsessional doubting circle, (represented by
the circle in our model), it is subjected to over-evaluation, fixation, worry,
distortion, amplification and misinterpretation. This weaponizes and escalates
the doubt and leads to significant emotional distress.
The
metacognitive processes of thinking about thinking, mean that the significance,
importance and impact of thoughts are
over-evaluated. OCD involves worry about the meaning of worry itself.
The process
of “Cognitive Fusion”, which is a core psychological process in Acceptance and
Commitment Therapy, is also a key driver
of obsessional doubt in the “Circle” stage of our model.
Fusion
causes thoughts to become sticky and caught up in attention and emotional
resistance. This increases the intensity and perceived seriousness or literal
meaning of thoughts. Fusion translates and classifies thoughts as facts or
realistic predictions, rather than loaded internal perceptions or judgements.
Research by
the International OCD Research foundation, has also identified a number of
OCD-related thinking patterns that validate and supercharge the primary doubt.
These
include Over-estimation of Threat, Thought Action Fusion, Perfectionistic
Thinking, Responsibility Bias, Uncertainty Intolerance and Catastrophizing.
These
thinking habits or distortions compound and exaggerate the worry, rumination
and self-questioning, leading to high levels of anxiety, shame, guilt,
embarrassment and disgust.
Obsessions
directly activate compulsive and avoidance behaviours in an attempt to gain
relief from the obsessional distress.
Repetitive
checking, avoidance, neutralizing, high-control and ritualistic behaviours are
commonly referred to as compulsions in OCD. In our model, compulsions are
represented in the “Square”.
Compulsions
can be external or “Overt” , such as checking locks and switches, excessive
cleaning, repeating and comparing.
Internal or
“Covert” compulsions can involve mental acts, rituals or routines such as
thought neutralizing, memory checking, the use of “cancelling” or “magic”
words, body scanning and sensory
checking.
Whilst
compulsions create a temporary sense of relief, outlined in the following
section on Operant and Conditioned learning, they also lead to significant
functional impairment.
OCD
compulsions and avoidance behaviours progressively interfere with the conduct
of normal daily life and consume significant amounts of time and energy. The
relentlessness of compulsions causes problems at work, at home and in key
personal relationships.
OCD is
reinforced by two important psychological processes known as Operant and
Conditioned learning.
These
processes create invisible psychological forces that maintain and validate the
OCD cycle. These forces are represented by the return arrows between the
“Circle” and the “Square”, and the arrow connecting the “Square” back to the
“Rectangle” at the top of the OCD cycle.
In our
model, the relationship between the obsessions and compulsions is represented
by the arrows labeled “Distress” and “Relief”.
Obsessional
doubts may for example, lead to feelings of anxiety and uncertainty about germs
or security. This distress is relieved through cleaning and checking
behaviours, also providing a temporary proxy for safety and control.
Operant
learning leads to engrained and
addictive compulsions by providing the elusion of immediate relief from the
obsessional doubt in the “Circle”.
Of course
the relief is not real, it is a proxy or temporary form of relief. The problem
is that this also inadvertently prevents the disconfirmation of the obsessional
doubt and creates an automatic association between the compulsion in the
“Square” and the trigger in the “Rectangle”.
This
association between the compulsion and the trigger is a process known as
“Conditioned Learning”, in which the trigger and compulsion become
automatically and tacitly associated.
Examples might include leaving the house
and automatically taking pictures of the lock, touching handles and using
sanitizer, seeing a vulnerable person and automatically scanning for feelings
of arousal.
This
association between the compulsion and the trigger eventually becomes so
intertwined, that individuals often report an awareness of the compulsion,
without consciously acknowledging the triggering event or situation.
This
process of association also reinforces the primary doubt implied by the
compulsion, which in turn maintains the vicious OCD cycle.
In this
way, OCD can be viewed as a three-part cycle, reinforced through a number of
faulty thinking processes and habitual behavioural patterns. The problem is
that for every increment of short-term relief or certainty gained through the
compulsion, OCD trades an increment of long-term reinforcement.
This trade-off
between relief and reinforcement leads to chronic psychological symptoms.
The purpose
of Cognitive and Behavioural Therapy is to learn new thinking and behavioural
techniques to break the cycle and establish healthy and adaptive coping
strategies.
These strategies include cognitive reappraisal of faulty thinking,
learning how to identify and unhook from obsessions, graded exposure to feared
situations and a process known as “Inhibitory Learning”.
These
strategies are covered under the section on Cognitive and Behavioural
treatment.
The first
step in this process and the purpose of this material, is to understand how OCD
is maintained in order to learn how to disrupt, break and replace the OCD cycle.